New research found that whether Ozempic works for you depends entirely on why you overeat and most doctors never ask that question

Ozempic has been one of the most talked about drugs on the planet for three years. Millions of people have taken it. Millions more are considering it. And a surprisingly large number of people who did take it are quietly confused about why it worked so well for their friend but barely moved the needle for them. A study from Japan just gave those people the most concrete answer they have received yet, and it reframes the entire conversation around why these drugs work the way they do.
The research tracked 92 people with type 2 diabetes in Japan across their first full year on GLP-1 medications including semaglutide, the active ingredient in Ozempic and Wegovy. Before the study began, each participant was assessed for their dominant eating pattern. What the researchers found after twelve months of follow-up was not a minor variation in outcomes. It was a clean split between two groups of people whose biology was responding to the same drug in fundamentally different ways.
The Drug Was Built for One Type of Overeating
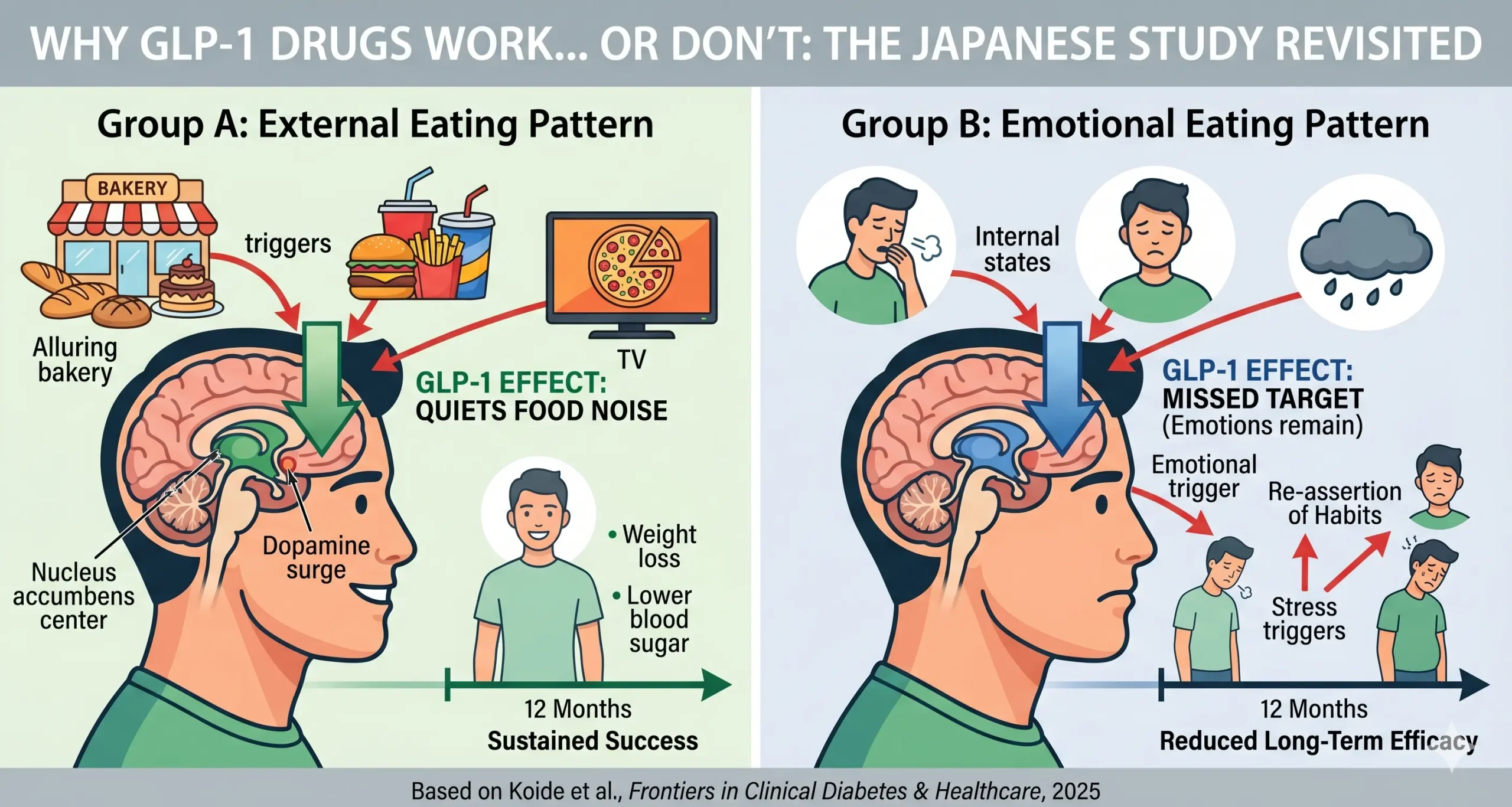
GLP-1 medications work primarily by suppressing the brain’s reward response to food. GLP-1s appear to dampen activity in reward-related regions like the nucleus accumbens, which plays a key role in cravings, dopamine release, and conditioned food responses. When someone on Ozempic says that food noise disappeared, that the constant mental chatter about what to eat next simply went quiet, they are describing the drug doing exactly what it was designed to do. It muffles the dopamine surge that the sight, smell, and anticipation of food normally triggers. Food becomes less compelling, not because the person is suppressing desire, but because the neurological machinery that generates that desire is being pharmacologically quieted.
This mechanism works beautifully for a specific category of overeating. People who tend to eat because tempting food looks or smells irresistible were much more likely to lose weight and improve blood sugar levels on GLP-1 medications. Researchers call this external eating, driven by environmental food cues rather than internal states. You walk past a bakery and something pulls you in. You see someone eating on screen and suddenly you are hungry. The drug intercepts exactly that pull, at the level of the dopamine circuit that generates it.
The People the Drug Was Not Built For
The other category is harder to address with a molecule that works on reward pathways. People who eat mainly in response to stress, sadness, or emotional struggles did not see the same long-term benefits.
Emotional eating is not primarily a reward-seeking behavior. It is a regulation behavior. People who eat in response to anxiety, depression, loneliness, or stress are not responding to a dopamine pull toward appealing food. They are using food to modulate an internal emotional state, to self-soothe, to create a temporary biochemical shift in how they feel. The mechanism driving that eating runs through different neural circuits than the ones GLP-1 drugs target.
Daisuke Yabe, a professor of medicine at Kyoto University and senior author of the study, framed it directly: GLP-1 receptor agonists are effective for individuals whose overeating is triggered by external stimuli. Their effectiveness is less expected when emotional eating is the primary cause. The drug quiets food noise. It does not quiet the emotional states that some people are using food to manage.
The participants in the external eating group sustained meaningful changes in their eating habits across the full twelve months of the study. The emotional and restrained eating groups had largely returned to their baseline patterns by the end of the year, despite taking the same medication at the same doses.
Why the Same Drug Produces Such Different Results
Understanding this split requires a brief look at what Ozempic is actually doing in the brain, because the marketing around these drugs has compressed a genuinely complex neurological story into a single phrase about appetite suppression.
GLP-1 receptors are distributed across multiple brain regions, not just the hypothalamus where hunger signals are regulated. They are heavily expressed in the nucleus accumbens and ventral tegmental area, the core structures of the brain’s reward and motivation system. In animals, dopamine release peaks after they eat a sweet meal, and after they are exposed to cocaine or opioids. But when there is a GLP-1 agonist onboard, that peak is pretty much squelched. This is why researchers are actively studying GLP-1 drugs as potential treatments for alcohol use disorder, nicotine addiction, and gambling disorders. The drug is not just suppressing hunger. It is dampening the reward salience of things the brain has learned to crave.
For someone whose overeating is driven by external food cues, this is exactly the intervention they needed. Their brain was overreacting to the sight and smell of food, generating an exaggerated dopamine response that drove consumption beyond any genuine need. Ozempic turns down that response directly.
For someone whose overeating is driven by emotional dysregulation, the dopamine pathway is not the primary problem. The eating is being recruited to manage cortisol, to create a temporary mood shift, to fill a psychological gap that has nothing to do with the rewarding appearance of food. Dampening the dopamine response to food cues does not address what is actually driving the behavior. The emotional state that triggers eating remains fully intact, and eventually the behavioral pattern reasserts itself.
What Nobody Checks Before Prescribing
This is where the clinical implications of the Japanese study become uncomfortable. The researchers’ recommendation was direct: healthcare professionals should assess a patient’s eating behavior patterns before prescribing these medications, and should consider treating underlying emotional eating patterns either alongside or before initiating GLP-1 therapy.
That is not what typically happens. The standard pathway to an Ozempic prescription involves blood sugar levels, BMI, and cardiovascular risk markers. Nobody asks whether a patient eats because cheese pizza looks incredible or because they had a brutal week at work. The distinction has not been part of the prescribing framework because the data to support it did not exist until recently.
The result is that a significant proportion of the people currently on GLP-1 drugs belong to the category the Japanese study identified as the poor responders. They take the medication, experience some initial benefit from the general appetite effects, and then gradually drift back toward their baseline eating patterns as the emotional drivers reassert themselves against a pharmacological mechanism that was never targeting them in the first place. When this happens, the conventional interpretation is that the drug stopped working or that the patient lacked discipline. Neither is accurate. The drug was doing what it does. It was just aimed at the wrong circuit.
The Question Worth Asking Before You Start
The Japanese study is observational and limited to 92 participants, all with type 2 diabetes in a single cultural context. It needs replication in larger and more diverse populations before it can change prescribing guidelines. But the biological framework it is pointing toward is grounded in well-established neuroscience and is consistent with what clinicians have been observing anecdotally for years.
GLP-1 drugs are genuinely transformative for the people they are designed for. For people whose weight and blood sugar problems are driven primarily by an overactive response to external food cues, the drugs deliver on almost every metric. The food noise disappears. The pull toward hyper-palatable food weakens. Eating becomes easier to manage because the brain’s reward machinery is no longer amplifying every food encounter into a compelling argument.
For people whose eating is doing emotional work, the same drug is addressing the wrong problem. The noise it quiets is not the noise that was driving the behavior. The researchers say that for this group, additional psychological support targeting emotional regulation should be considered alongside any pharmacological intervention.
The question is not whether Ozempic works. The question is what kind of overeating a person actually has. And right now, most people taking these drugs have never been asked.
Source:
Koide, Y., Kato, T., Hayashi, M., et al. Association between eating behavior patterns and the therapeutic efficacy of GLP-1 receptor agonists in individuals with type 2 diabetes: a multicenter prospective observational study. Frontiers in Clinical Diabetes and Healthcare, July 4, 2025. DOI: 10.3389/fcdhc.2025.1638681 https://www.frontiersin.org/journals/clinical-diabetes-and-healthcare/articles/10.3389/fcdhc.2025.1638681/full