Scientists found that people taking Ozempic face more social judgment than people who stay obese and the data explains why millions are hiding their prescriptions


Millions of people have lost significant weight on Ozempic and Wegovy. Many of them are not telling anyone how they did it. Two studies published in spring 2026 by researchers at Rice University, Georgetown, Mayo Clinic, and UCLA have now documented the reason in data, and it is more counterintuitive than most people expect.
People who lose weight using GLP-1 medications may actually face more judgment than those who lose weight through diet and exercise, or even those who don’t lose weight at all. The social penalty for using a drug to treat obesity is, in measurable terms, larger than the social penalty for staying obese. This is the double bind that tens of millions of people are quietly navigating, and neither the medical establishment nor the public conversation around these drugs has adequately reckoned with it.
The Study That Surprised Its Own Researchers
Erin Standen, assistant professor of psychological sciences at Rice University, designed the study expecting to find some stigma around GLP-1 use. “We expected there might be some stigma around using a GLP-1,” Standen said. “But what surprised us was the extent of it.”
The Rice study, published in the International Journal of Obesity, tested how people judge different weight-loss paths. Participants were shown scenarios describing individuals who had lost the same amount of weight through different means, diet and exercise, GLP-1 medication, or who had not lost weight at all. The judgments that came back were not neutral assessments of health outcomes. They were moral evaluations, and the moral mathematics produced a result that defies the logic of weight loss as a purely medical issue.
Losing weight on Ozempic generated more negative judgment than not losing weight at all. The act of treating a medical condition with a medically approved treatment was viewed more harshly than simply having the condition without intervention. “There’s this idea that if you lose weight, you might escape stigma,” Standen said. “But what we’re seeing is that people may face judgment at multiple points. They may be judged for their weight and for how they choose to manage it.”
The Easy Way Out Narrative
The mechanism driving this social penalty is not mysterious. “There’s a narrative that using these medications is ‘taking the easy way out,'” Standen said. This narrative frames weight loss as a moral achievement that requires suffering, restriction, and demonstrated willpower. Under this framework, diet and exercise produce weight loss that counts as earned, while medication produces weight loss that does not, regardless of the health outcomes being identical or better on the pharmacological route.
The Georgetown study, published in Stigma and Health, added granularity to this picture. Researchers recruited 402 participants and presented them with scenarios involving women who had lost weight using GLP-1 drugs versus lifestyle interventions. Women who use these drugs for weight loss face significantly more judgment than those who lose weight through diet and exercise, and this stigma was driven primarily by the perception that medication is an easy way out.
The stigma was not merely social disapproval expressed in conversation. “Our results show that the ‘easy way out’ perception does more than spark casual criticism. It can translate into measurable stigma, including fat phobia and a desire for social distance,” said lead researcher Stacy Post, a postdoctoral researcher at Georgetown’s Lombardi Comprehensive Cancer Center.
People who had lost weight on GLP-1 drugs were rated as less worthy of admiration and less deserving of social connection than people who had lost the same weight through diet and exercise. The weight loss itself was not the variable that mattered. The story of how it happened was.
The Racial Dimension Nobody Expected
One of the more striking findings from the Georgetown study involves race. The stigma was more pronounced when the person using the drug was portrayed as white rather than Black. White women using GLP-1 drugs were more frequently accused of taking a shortcut, which in turn fueled greater social rejection. Notably, both Black and white study participants tended to view GLP-1 use as a shortcut similarly.
The researchers suggest this disparity may reflect different social narratives about willpower and body image that operate differently across racial groups in American culture. White women using GLP-1 drugs were perceived as having access to a shortcut they should not have needed, while the same judgment was less frequently applied to Black women in identical scenarios. The stigma is not race-neutral, and the social experience of using these drugs is not uniform across the populations who are clinically eligible for them.
What Happens When the Weight Comes Back
The Rice study extended its analysis to examine what happens when people regain weight after stopping GLP-1 medication, a common outcome given that the drugs need to be taken continuously to maintain their effects. The findings were even more punishing than the initial stigma results.
People who regained weight after discontinuing a GLP-1 drug faced significantly more social judgment than people who regained weight after stopping a diet and exercise plan, or even people who had never lost weight at all. The narrative around relapse on medication was interpreted as a moral failure compounded by having taken a shortcut in the first place. Every stage of the medication journey, starting it, losing weight on it, stopping it, and regaining weight after stopping, came with its own layer of social penalty that the equivalent stages of a lifestyle-based weight loss attempt did not.
This is the full picture of what the researchers are calling the GLP-1 paradox. A person with obesity who uses a medically proven treatment faces more social rejection than a person with obesity who uses no treatment at all, and more rejection still if the treatment eventually stops working in the way most obesity treatments eventually do.
The Clinical Consequence
The social stigma documented in these studies is not just an interpersonal discomfort. It has measurable consequences for whether people seek treatment at all. Health experts say the growing stigma and shame surrounding the use of drugs like Ozempic and Wegovy may keep those who need them most from seeking treatment.
More than 100 million people in America are clinically eligible to use GLP-1 medications for weight loss, and approximately 18% of US adults are currently using or have previously used a GLP-1 drug. The gap between eligibility and use is partly economic, partly logistical, and partly driven by exactly the social dynamic these studies are measuring. People who would benefit medically from these treatments are weighing that benefit against the social cost of being perceived as having taken the easy way out, and a significant number of them are deciding the social cost is too high.
“GLP-1 medications can offer meaningful health benefits for people with obesity, but many patients report feeling shame and guilt for using them,” Post said. That shame is not a personal weakness or an irrational response. It is a predictable reaction to a documented social environment in which the medical treatment of a chronic disease has been culturally reframed as a character failure.
The Assumption Underneath the Judgment
The easy way out framing that drives all of this stigma rests on an assumption that has been consistently contradicted by decades of obesity research: that body weight is primarily a matter of individual willpower, and that people who are obese have simply not tried hard enough through legitimate means.
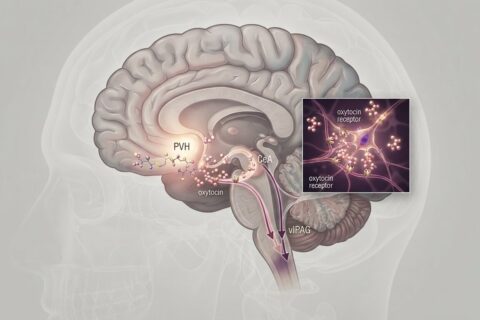
The biological reality is that body weight is regulated by genetics, hormonal systems, gut microbiome composition, sleep patterns, stress hormones, and dozens of other factors that operate largely outside conscious control. GLP-1 medications work because they correct a biological signaling deficit, not because they substitute for effort that the person was capable of making. The previous Ozempic article we wrote documented precisely this: the drugs target the brain’s dopamine response to food cues, addressing a neurological mechanism that has nothing to do with discipline.
The judgment these drugs attract is therefore not a judgment about what the person did or failed to do. It is a judgment based on a model of obesity that the science has largely abandoned while the culture has not caught up. The people quietly hiding their Ozempic prescriptions from friends and family are not ashamed of being weak. They are navigating the distance between what medicine now knows about their condition and what the people around them still believe.
Sources:
1. Rice University / International Journal of Obesity, May 2026 Standen, E., Phelan, S., Tomiyama, J. An experimental investigation of the stigmatization of weight loss and regain from GLP-1 receptor agonist use and cessation. International Journal of Obesity, 2026. DOI: 10.1038/s41366-026-02061-y https://www.nature.com/articles/s41366-026-02061-y
2. Georgetown / George Washington University, Stigma and Health, April 2026 Post, S.M., Stock, M.L., Persky, S. Comparing the impact of GLP-1 agonists vs. lifestyle interventions and weight controllability information on stigma and weight-related cognitions. Stigma and Health, April 9, 2026. https://lombardi.georgetown.edu/news-release/new-study-examines-stigma-toward-women-who-lose-weight-using-glp-1-medications/